The Feminine Mystaque:
Second-Wave Feminism’s Contributions to Rising Rates of ADHD and Autism
Abstract
In the 1990s, diagnoses of the mental disorders ADHD and autism increased drastically. Several theories came forth to attempt to explain the disturbing increase. This paper explains how the social changes that resulted from the Second Wave of American Feminism contribute to these increasing rates. A mental disorder can be seen as a trait that is so disadvantageous, it inhibits a person from normal, independent functioning. This makes the diagnosis of a mental disorder subject to culture, since culture dictates which traits are embraced or rejected. ADHD and autism are comprised of extreme versions of male traits, and the elevation of women caused these traits to fall out of favor. This falling out of favor made day to day functioning difficult for those who possess those traits, leading those traits to now be identified as mental disorders. There may be actual changes in the prevalence of the traits in question, but such arguments have thus far failed to present comprehensive evidence demonstrating that changes in prevalence are responsible for the radical increase in diagnoses. Thus, a change in attitude toward masculine traits is the most reasonable explanation for increasing ADHD and autism rates.
Introduction
An unprecedented epidemic of mental disorders arose in the United States in the 1990s when diagnoses of ADHD and autism skyrocketed sevenfold in ten short years. This controversial phenomenon was far from the only issue gripping the American people- the Soviet Union was dissolving, the Gulf War raged, and global warming debates intensified. Women’s Rights activists made social changes at an unforeseen rate. An unexpected connection lies between the latter and the former- The social changes that resulted from the Second Wave of American Feminism significantly contributed to the puzzlingly high rates of ADHD and autism.
Background
The goals of the Feminist movement are fairly straightforward. The movement sought to eliminate inequality between men and women that had existed for millennia before. In both the public and private spheres, women sought greater influence in a culture they argued was geared against them. Unequivocally, they succeeded- politically, socially, educationally, and otherwise. While its precise outcomes vary in nature from case to case, each shares one common element- being a female no longer carried the disadvantages it always did. By the same coin, being a female was now more favorable than it ever was.
Attention-Deficit Hyperactivity Disorder is a commonly diagnosed mental disorder that comes in two primary varieties. Inattentive, formerly known as Attention Deficit Disorder, or ADD, is characterized by inactivity and “spaceyness”. Hyperactive is characterized by constant movement and fidgeting. Those being the primary differences, both are characterized by the inability to focus attention for extended periods of time.
Autism is a mental disorder that varies in presentation and severity. Along with Asperger syndrome, the two form the majority of pervasive developmental disorders, or PDDs, which are referred to as autism in lay terms. PDDs are characterized by impaired social function and communication skills, resistance to changes in routine, and strong interest in non-social activities.
Beginning in the 1990’s, diagnostic rates of ADHD shot up dramatically. In 1970, an estimated 1.2% of schoolchildren were treated for ADHD. By 2007 estimates state up to 16% of schoolchildren received treatment (National Health Service, 2008). Autism rates have similarly skyrocketed. In 1996, 0.7 out of 1,000 children were diagnosed with autism. By 2007, that number multiplied nearly eightfold to an astounding 5.2 out of 1,000 (Wing, Potter, 2002). This unsettling rise in diagnoses has made the two disorders some of the most controversial social issues of the past decade and a multitude of opinions regarding the rise have arisen. Opinions range from claims that both disorders are inventions, to claims that that the actual prevalence of the diseases are higher than their diagnostic rates and they have been merely unaddressed in the past.
Psychological Illnesses
All mental disorders carry a unique quality- they reflect the culture they occur in. It is difficult to draw the line between a personality trait and a disease of the mind- the same trait in one culture may be seen as energetic curiosity, but it may be Bipolar disorder in another, for example. All mental disorders carry a universal qualifier- Does the trait hinder an individual from functioning normally in daily life? By this reasoning, any extreme personality trait may constitute a mental disorder. While any given personality trait is objectively definable, in order to achieve status as a mental disorder, the trait must be such a disadvantage to the individual that it hinders an individual from normal, independent functioning.
An individual’s capacity to function independently depends heavily upon the culture he or she lives in. A trait may be embraced and nurtured, or it may be discouraged and stigmatized. When the latter happens in sufficient magnitude, an individual is then hindered from living a typical life. How much a culture favors a personality trait can be known as trait favorability, or simply favorability.
This makes any such diagnosis subjective- the ability to function independently is entirely dependent upon the culture the individual lives in. Thus, if a culture changes, previously permissible traits would become accordingly disadvantageous. The influence of trait favorability is reflected in radically differing rates between different cultures. If cultural changes can be accurately tracked, changes in diagnoses of mental disorders can be independently predicted. Thus, two main factors can be said to contribute to the diagnosis of a mental disorder: the trait and its favorability.
Autism
Autism is a mental disorder characterized by impaired communication and socialization, preoccupation with organization and categorizing, and an overall delay in normal childhood development. Most autistic individuals are males- approximately four males are diagnosed for every one female. Not surprisingly, most components of autism have been shown to be distinctly masculine traits that occur commonly in non-autistic males, only lesser in magnitude. Such a hypothesis has been formulated, called the “extreme male brain theory” of autism (Baron-Cohen, S., et al, 2005).
By numerous metrics, males have demonstrated a preference for “systemizing” over “empathizing”. That is, males show stronger interest in “systems”, which are defined as anything that follows rules, which are defined as repeating, lawful patterns. This is contrasted to empathizing, which is defined as the drive to identify a person’s thoughts and feelings and to respond with an appropriate emotion (Baron-Cohen, S, et al, 2005).
Figure 1 illustrates the alarming rise in autism diagnoses from 1996 to 2007. Such a statistic raises the question of whether the increase is due to an actual increase in the prevalence of the traits that comprise autism, or if it is the result of a change in those traits’ favorability.
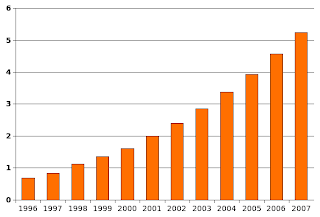

Figure 1. Autism diagnoses per 1,000 children in the United States (Wing, Potter, 2002)
ADHD
ADHD is a mental disorder characterized by either “spaceyness” (Inattentive subtype) or hyperactivity (Hyperactive subtype), and a marked inability to focus for extended periods of time. Diagnostic rates vary greatly from region to region, ranging from 2-16% of schoolchildren (Rader, McCauley, Callen, 2009). Boys with ADHD outnumber girls four to one (Singh, 2008).
Several researchers have used neuroimaging, or brain scan studies to correlate ADHD with marked differences in brain anatomy and activity. Castellanos found that ADHD brains were smaller in volume than non-ADHD brains, with a proportionally greater reduction in volume in the left pre-frontal cortex, which has been independently established to play a role in “executive functioning” (1996). Executive functioning is the “master” function that coordinates the utilization of all other cognitive functions, and without this coordination an individual becomes impulsive and disinhibited. Bruhn found differences in the level of neurotransmitter activity in certain regions of the brain, namely the striatum, which is implicated in advance planning (1989). Zametkin found that ADHD patients had lower dopamine levels across the board (1986). All these differences are accountable by the known differences between male and female brains. A hyperactive state is thought to be an evolutionary adaptation that is “left over” from ancestors who hunted animals to survive (Hartmann, 1995). Males mature later than females in most aspects of development. The left prefrontal cortex is no exception, and it takes several more years to fully develop in males than in females, possibly accounting for its reduced size found in ADHD patients (Garn, 1992) and the subsiding of ADHD into adulthood in approximately 40% of childhood cases (Valdizan, 2009).
Feminism: Second-Wave
The American Second-Wave Feminist movement was a broad and powerful movement that sought to increase women’s influence in nearly every layer of the American culture. While disputes among Feminists were often greater than their disputes with the culture they sought to change, all proponents argued that men unjustly exercised control over women in a variety of ways. In spite of this internal tension, women were significantly empowered in the social, political, and educational spheres. The universal outcome of the movement was that womanhood was an unprecedentedly favorable trait.
Prior to the movement, traditional gender roles were strongly enforced. According to Woolf (1920), men took the roles of breadwinner and head of house, while women took the role of childrearing and homemaking. Men were expected to pursue careers that would provide for a comfortable standard of living for his wife and children. Women were expected to devote their time to home life. Men were portrayed as being more stoic, quick to express anger, easily overwhelmed by expressions of emotion, and driven to dominate. Women were portrayed as emotionally expressive, empathetic, sensitive, and passive.
Feminists saw these roles as subjugating and oppressive. In her 1963 book The Feminine Mystique, often credited with sparking the Second Wave of American Feminism, Betty Friedan argued that traditional gender roles and their accompanying stereotypes made women second-class citizens in a male-dominated culture by offering women no other role than wife and mother. She encouraged women to adopt roles in traditionally male-dominated areas, namely education and the workplace.
For these reasons, attempts were made to correct for the unequal treatment of women in education and the workplace. Numerous laws were passed requiring public educational institutions to admit certain amounts of women, or requiring companies to hire certain amounts of women. Accordingly, women entered the public sphere and found themselves in places of authority they had never previously found themselves in.
Argument
As previously discussed, a change in the favorability of a certain trait would alter diagnostic rates of disorders comprised of those traits. The Feminist movement empowered women, and accordingly, femininity increased in favorability. By the same token, masculinity decreased in favorability. Therefore, diagnostic rates of mental disorders comprised of masculine traits would increase accordingly-namely, ADHD and autism. The stigmatization of masculine traits to the point of diagnosing up to 16% of males as disabled brings in to question how much the Feminist movement actually resulted in elimination, rather than reversal, of prejudiced attitudes.
Opposing view
Some may take issue with the assumption that males and females have fundamentally different psychological traits. In fact a fundamental goal of the Feminist movement was to eliminate gender stereotypes. Unfortunately, the claim that gender plays no role in an individual’s traits is completely unsubstantiated by any empirical observation whatsoever. Differences between male and female brains are well documented, although the interpretation of those differences has been less than clear, such as Paul Broca’s hasty and unscientific conclusions about the inferiority of female intelligence.
The traits of autism are beginning to be accounted for by genetic studies. A number of genes found on the X chromosome have accounted for roughly 20% of its heritable component (Benvenuto, et al, 2009). The fact that it is found on the X chromosome explains why it is such a distinctly male trait- males have one X and one Y chromosome, whereas females have two X chromosomes. What this means is in order for a female to have a trait, the same version of the gene must be found on both X chromosomes, while males only require one copy on the X chromosome. It is much less likely for an individual to acquire two copies of the same gene rather than one, so males would therefore be much more likely to express the trait than females.
Opponents may further argue that gender-specific traits only arise because individuals are only ever expected to have those traits. This assertion certainly poses an interesting chicken-egg problem, but it in fact does not disprove anything. While the traits may have arisen out of societal expectation, the traits nonetheless exist, and their reality cannot be argued against. In the case that traits arise out of expectation, it would only further incriminate the Feminist movement by demonstrating that it failed to eliminate gender stereotypes, continued their enforcement, and reversed discrimination from female to male traits. That being said, there is no reason to believe that is the case.
It is possible for the increase in diagnoses to be the result of an actual increase in the prevalence of the traits, rather than the same traits being viewed in a different light. Such a change in the actual trait prevalence would require an unimaginably rapid shift in genetics- a rate that has yet to ever be observed, that is probably impossible. Currently, there is an utter lack of compelling evidence in favor. While this explanation remains a possibility, there is no reason to assume changes in the traits’ prevalence contribute significantly until more comprehensive evidence is presented.
Conclusion
The unsettling rises in ADHD and autism rates are sociological in origin. In accordance with the fallout of a movement centered on women, the American social and cultural environment geared itself toward women, making their defining traits more favorable. This increase in feminine favorability reduced the favorability of masculine traits, making those possessing such traits disadvantaged in a way they wouldn’t be were it not for the Feminist movement. This disadvantage made extreme versions of the trait amenable to being called a disorder because of their incapacitating effects upon anyone who possesses them. ADHD and autism are distinctly masculine both in terms of the traits that comprise them, and actual diagnostic rates between the sexes. In accordance with the former prediction, diagnostic rates of the masculine disorders ADHD and autism increased dramatically in a world that is hostile to their comprising traits.
References
Benvenuto, A., Manzi, B., Alessandrelli, R., Galasso, C., Curatolo, P., (2009). Recent Advances in the Pathogenesis of Syndromic Autisms International Journal of Pediatrics
Bruhn, Henriksen L, Lou, et al. (2011). Striatal dysfunction in attention deficit and hyperkinetic disorder. Arch Neurol 46:48-52
Castellanos, F. Xavier, Giedd, Jay N. Marsh , Wendy L., Hamburger, Susan D, Vaituzis , A. Catherine, Dickstein , Daniel P,Sarfatti , Stacey E,Vauss, Yolanda C,Snell , John W,Lange , Nicholas, Kaysen , Debra, Krain , Amy L, Ritchie , Gail F,Rajapakse, Jagath C, Rapoport, Judith L., (1996). Quantitiative brain magnetic resonance imagining in attention-deficit hyperactivity disorder. Arch Gen Psychiatry, 53 (7), 607-16
Friedan, B. (1963). The Feminine Mystique W. W. Norton & Company
Garn, S.M., (1992). Physical growth and development. Comprehensive Adolescent Health Care
Garn, SM. (1992). Physical growth and development. In: Friedman SB, Fisher M, Schonberg SK., editors. Comprehensive Adolescent Health Care. St Louis: Quality Medical Publishing
Hartmann, T. (1995). ADD Success Stories Underwood Books
Mulrine, A. (2001). Are Boys the Weaker Sex? U.S. News & World Report, 131 (4), 40-48.
National Health Service (2008). Attention deficit hyperactivity disorder (ADHD): full guideline
Rader, R., McCauley, L., Callen, E.C., (2009), Current strategies in the diagnosis and treatment of childhood attention-deficit/hyperactivity disorder. Am Fam Physician, 79 (8): 657-65
Singh, I., (2008). Beyond polemics: science and the ethics of ADHD. Nature Reviews. Neuroscience, 9 (12): 957-64
Valdizán, J.R., Izaguerri-Gracia, A.C., (2009). Attention deficit hyperactivity disorder in adults. Revista de neurologia 48 Suppl 2: S95–9.
Wing, L., Potter, D., (2002). The epidemiology of autistic spectrum disorders: is the prevalence rising? Ment Retard Disabil Res Rev, 8 (3): 151-61
Woolf, Virginia. (1929). A Room of One’s Own p. 76
Zametkin, A.J., Rapaport J.L., Murphy D.L., (1986). Treatment of hyperactive children with monoamine oxidase inhibitors, I: clinical efficacy. Arch Gen Psychiatry, 42: 962-66